Cure For Bursitis Of The Feet
Overview
Retrocalcaneal bursitis is closely related to Haglund?s Deformity (or ?pump bumps?). If you have a bony enlargement on the back of the heel that rubs the Achilles tendon, it can cause the formation of a bursa (small fluid filled sack). It usually happens in athletes as shoes rub against the heel. The bursa can aggravated by the stitching of a heel counter in the shoe as well. It can make wearing shoes and exercising difficult. Another term used for this condition is ?pump bump? because it can frequently occur with wearing high heels as well. ?Retro-" means behind and ?calcaneus? means heel bone. So this is precisely where the bursitis (inflammation of the bursa) develops. Once it begins and you develop bursitis between the heel bone and the Achilles tendon, it can become even more painful. When most people first notice retrocalcaneal bursitis, it is because the skin, bursa and other soft tissues at the back of the heel gets irritated as the knot of bone rubs against the heel counter in shoes. The back of the shoes create friction and pressure that aggravate the bony enlargement and pinches the bursa while you walk.
Causes
Bursitis, tendinitis, and other soft tissue rheumatic syndromes typically result from one or more factors. These include: Play or work activities that cause overuse or injury to the joint areas Incorrect posture Stress on the soft tissues from an abnormal or poorly positioned joint or bone (such as leg length differences or arthritis in a joint) Other diseases or conditions (rheumatoid arthritis, gout, psoriasis, thyroid disease, or an unusual drug reaction) Infection.
Symptoms
Retrocalcaneal bursitis is very similar to Achilles bursitis as the bursae are very close in proximity and symptoms are almost identical however retrocalcaneal bursitis is a lot more common. The symptoms of bursitis vary depending on whether the bursitis is the result of injury or an underlying health condition or from infection. From normal overuse and injury the pain is normally a constant dull ache or burning pain at the back of the heel that is aggravated by any touch, pressure like tight shoes or movement of the joint. There will normally be notable swelling around the back of the heel. In other cases where the bursa lies deep under the skin in the hip or shoulder, swelling might not be visible. Movement of the ankle and foot will be stiff, especially in the mornings and after any activity involving the elbow. All of these symptoms are experienced with septic bursitis with the addition of a high temperature of 38?C or over and feverish chills. The skin around the affected joint will also appear to be red and will feel incredibly warm to the touch. In cases of septic bursitis it is important that you seek medical attention. With injury induced bursitis if symptoms are still persisting after 2 weeks then report to your GP.
Diagnosis
The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis.
Non Surgical Treatment
Treatment is primarily comprised of relief from the painful activity (running). It is important that shoes do not pinch the heel. If satisfactory progress is not made during the rehabilitation, medical treatment can be considered in the form of rheumatic medicine (NSAID) or injection of corticosteroid in the bursa. Injections should be performed under ultrasound guidance to ensure optimal effect and reduce the risk of injecting into the Achilles itself. If progress is not made neither through rehabilitation nor medicinal treatment, surgical treatment can be attempted.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Retrocalcaneal bursitis is closely related to Haglund?s Deformity (or ?pump bumps?). If you have a bony enlargement on the back of the heel that rubs the Achilles tendon, it can cause the formation of a bursa (small fluid filled sack). It usually happens in athletes as shoes rub against the heel. The bursa can aggravated by the stitching of a heel counter in the shoe as well. It can make wearing shoes and exercising difficult. Another term used for this condition is ?pump bump? because it can frequently occur with wearing high heels as well. ?Retro-" means behind and ?calcaneus? means heel bone. So this is precisely where the bursitis (inflammation of the bursa) develops. Once it begins and you develop bursitis between the heel bone and the Achilles tendon, it can become even more painful. When most people first notice retrocalcaneal bursitis, it is because the skin, bursa and other soft tissues at the back of the heel gets irritated as the knot of bone rubs against the heel counter in shoes. The back of the shoes create friction and pressure that aggravate the bony enlargement and pinches the bursa while you walk.
Causes
Bursitis, tendinitis, and other soft tissue rheumatic syndromes typically result from one or more factors. These include: Play or work activities that cause overuse or injury to the joint areas Incorrect posture Stress on the soft tissues from an abnormal or poorly positioned joint or bone (such as leg length differences or arthritis in a joint) Other diseases or conditions (rheumatoid arthritis, gout, psoriasis, thyroid disease, or an unusual drug reaction) Infection.
Symptoms
Retrocalcaneal bursitis is very similar to Achilles bursitis as the bursae are very close in proximity and symptoms are almost identical however retrocalcaneal bursitis is a lot more common. The symptoms of bursitis vary depending on whether the bursitis is the result of injury or an underlying health condition or from infection. From normal overuse and injury the pain is normally a constant dull ache or burning pain at the back of the heel that is aggravated by any touch, pressure like tight shoes or movement of the joint. There will normally be notable swelling around the back of the heel. In other cases where the bursa lies deep under the skin in the hip or shoulder, swelling might not be visible. Movement of the ankle and foot will be stiff, especially in the mornings and after any activity involving the elbow. All of these symptoms are experienced with septic bursitis with the addition of a high temperature of 38?C or over and feverish chills. The skin around the affected joint will also appear to be red and will feel incredibly warm to the touch. In cases of septic bursitis it is important that you seek medical attention. With injury induced bursitis if symptoms are still persisting after 2 weeks then report to your GP.
Diagnosis
The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis.
Non Surgical Treatment
Treatment is primarily comprised of relief from the painful activity (running). It is important that shoes do not pinch the heel. If satisfactory progress is not made during the rehabilitation, medical treatment can be considered in the form of rheumatic medicine (NSAID) or injection of corticosteroid in the bursa. Injections should be performed under ultrasound guidance to ensure optimal effect and reduce the risk of injecting into the Achilles itself. If progress is not made neither through rehabilitation nor medicinal treatment, surgical treatment can be attempted.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Hammer Toe Surgery Procedure
 Overview
Overview
A hammertoe is a deformity of the second, third or fourth toe in which the toe becomes bent at the middle joint; hence, it resembles a hammer. Claw toe and mallet toe are related conditions. While a hammer toe is contracted at the first toe joint, a mallet toe is contracted at the second toe joint, and a claw toe is contracted at both joints. According to the 2012 National Foot Health Assessment conducted by the NPD Group for the Institute for Preventive Foot Health, 3 percent of U.S. adults age 21 and older (about 7 million people) have experienced hammer toe or claw toe. The condition is significantly more prevalent in females than in males.
Causes
It is possible to be born with a hammer toe, however many people develop the deformity later in life. Common causes include tightened tendons that cause the toe to curl downward. Nerve injuries or problems with the spinal cord. Stubbing, jamming or breaking a toe. Having a stroke. Being a diabetic. Having a second toe that is longer than the big toe. Wearing high heels or tight shoes that crowd the toes and don?t allow them to lie flat. Aging.
 Symptoms
Symptoms
Well-developed hammertoes are distinctive due to the abnormal bent shape of the toe. However, there are many other common symptoms. Some symptoms may be present before the toe becomes overly bent or fixed in the contracted position. Often, before the toe becomes permanently contracted, there will be pain or irritation over the top of the toe, particularly over the joint. The symptoms are pronounced while wearing shoes due to the top of the toe rubbing against the upper portion of the shoe. Often, there is a significant amount of friction between the toe and the shoe or between the toe and the toes on either side of it. The corns may be soft or hard, depending on their location and age. The affected toe may also appear red with irritated skin. In more severe cases, blisters or open sores may form. Those with diabetes should take extra care if they develop any of these symptoms, as they could lead to further complications.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
The treatment options vary with the type and severity of each hammertoe, although identifying the deformity early in its development is important to avoid surgery. Podiatric medical attention should be sought at the first indication of pain and discomfort because, if left untreated, hammertoes tend to become rigid, making a nonsurgical treatment less hammertoe of an option. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Surgical Treatment
Sometimes when the joints are removed the two bones become one as they are fused in a straightened position. Many times one toe will be longer than another and a piece of bone is removed to bring the toes in a more normal length in relation to each other. Sometimes tendons will be lengthened, or soft tissue around the joints will be cut or rebalanced to fix the deformity. Angular corrections may also be needed. The surgeon may place fixation in your foot as it heals which may include a pin, or wires.
Do Hammer Toe Braces Work
 Overview
Overview
A Hammer toes is a deformity of the second, third or fourth toes in which the main toe joint is bent upward like a claw. Initially, hammertoes are flexible and can be corrected with simple measures. Left untreated, they can become fixed and require surgery. Hammertoe results from shoes that don?t fit properly or a muscle imbalance, usually in combination with one or more other factors. Muscles work in pairs to straighten and bend the toes. If the toe is bent and held in one position long enough, the muscles tighten and can?t stretch out.
Causes
But what causes the imbalance of the tendons and muscles in the first place so that they begin to pull and bend the joint? A bad fitting shoe could be the cause but it usually isn?t the primary cause. Many people are genetically predisposed to hammertoe, and the condition begins to progress more quickly when they wear shoes that fit poorly, for example pointy toes, high heels, or shoes that are too short. Hammertoe may also be caused by damage to the joint as a result of trauma.
 Symptoms
Symptoms
The most obvious symptom of hammer, claw or mallet toe is the abnormal toe position. This is usually combined with pain: the abnormal foot position leads to excessive friction on the toe as it rubs against any footwear which can be extremely painful. Corns & Calluses: repeated friction can result in the formation of a foot corn or callus on top of the toes. Stiffness, the joints become increasingly stiff. In the early stages, the toes can usually be straightened out passively using your hands, but if allowed to progress, the stiffness may be permanent.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe.
Non Surgical Treatment
Your podiatrist may recommend conservative treatment techniques for your hammertoes based on your foot structure, which will likely involve removing any thick, painful skin, padding your painful area, and recommending for you shoes that give your curled toes adequate room. Conservative care strategies for this health purpose may also involve the use of Correct Toes, our toe straightening and toe spacing device.
Surgical Treatment
If your hammer, claw, or mallet toe gets worse, or if nonsurgical treatment does not help your pain, you may think about surgery. The type of surgery you choose depends on how severe your condition is and whether the toe joint is fixed (has no movement) or flexible (has some movement). A fixed toe joint often requires surgery to be straightened. A flexible toe joint can sometimes be straightened without surgery. Surgery choices include Phalangeal head resection (arthroplasty), in which the surgeon removes part of the toe bone. Joint fusion (arthrodesis), in which the surgeon removes part of the joint, letting the toe bones grow together (fuse). Cutting supporting tissue or moving tendons in the toe joint. How well surgery works depends on what type of surgery you have, how experienced your surgeon is, and how badly your toes are affected.
 Prevention
Prevention
The best first step you can take is to hammertoes evaluate your shoe choices. Ditch any shoes that aren?t serving your feet well. Shoes that crowd the front of your foot, especially around your toes, aggravate the existing condition and can also cause the condition to develop. If you suspect the development of hammertoe, you may also try using protective pads to prevent irritation and the development of corns. Custom orthotics to correct muscle imbalances in your feet may also help prevent hammertoe.
Hallux Valgus Deformity Symptoms
Overview
 A bunion is a firm, fluid-filled pad overlying the inside of the joint at the base of the big toe (metatarsophalangeal joint). The pad (bursa), which may get larger and stick out, can become inflamed and painful. Bunions may run in families, but many result from wearing tight shoes. Nine out of 10 bunions are developed by women. Nine out of 10 women wear shoes that are too small. Tight shoes also can cause other disabling foot problems like corns, calluses and hammertoes.
A bunion is a firm, fluid-filled pad overlying the inside of the joint at the base of the big toe (metatarsophalangeal joint). The pad (bursa), which may get larger and stick out, can become inflamed and painful. Bunions may run in families, but many result from wearing tight shoes. Nine out of 10 bunions are developed by women. Nine out of 10 women wear shoes that are too small. Tight shoes also can cause other disabling foot problems like corns, calluses and hammertoes.
Causes
Bunions are the byproduct of unnatural forces and motion being applied to the joints and tendons of your foot over a prolonged period of time. They can also be caused by traumas to the foot as well as congenital deformities. Occupations or athletic activities that place abnormal stress on your feet can also lead to the formation of bunions. Bunions have a tendency to run in families, but it?s not the bunion itself that is hereditary. It?s the the foot type which *causes* the bunion that is hereditary. Also, wearing shoes such as high heels that do not distribute your body weight evenly can lead to bunions, which explains why so many women suffer from bunions.
Symptoms
Alteration in alignment of the first toe. Pain in the 1st toe joint with movement. Restriction in range of demi pointe. Inflammation of the 1st toe joint. Rotation of the big toe so that the nail no longer faces upwards. Occasionally bruising of the toe nail occurs.
Diagnosis
Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment.
Non Surgical Treatment
Treatment options are based on the severity of the deformity and symptoms. Nonsurgical treatments usually are enough to relieve the pain and pressure on the big toe. Your doctor may tell you to start wearing roomy, comfortable shoes and use toe padding or a special corrective device that slips into your shoes to push the big toe back into its proper position. To help relieve pain, you can take over-the-counter medications such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin and others). Whirlpool baths also may help to ease discomfort. 
Surgical Treatment
Bunion surgery is most often performed as an out-patient, this means you go home that same day. It will likely be done at a hospital or out-patient (ambulatory) surgery center. The anesthetic choices with bunion surgery are local with sedation, spinal or general anesthesia. You wouldn?t expect that a small bunion would be treated exactly the same as a large one. Over the years, surgeons have developed dozens of methods to surgically correct bunions. But don?t worry because only a handful of methods are used today. With most bunion surgeries today, the procedure involves a combination of soft-tissue rebalancing of ligaments and tendons as well as bone work to re-align the foot structure. You may have heard people say they had their ?bunion shaved.? In most cases, the surgery often involves much more than simply shaving the bunion. The shaving part of the procedure is called an ?exostectomy? and often performed in conjunction with other methods.
The Treatment Of Over-Pronation Of The Feet
Overview
The problem with pronation is when it is excessive, here the term overpronation (or hyper-pronation) is used. This is quite a common problem and can lead to a number of injuries, especially in runners, including shin splints, anterior compartment syndrome, patello-femoral pain syndrome, plantar fasciitis, tarsal tunnel syndrome, bunions (Hallux valgus) and achilles tendonitis..jpg)
Causes
A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development.
Symptoms
Because overpronation affects the entire lower leg, many injuries and conditions may develop and eventually cause problems not only in the leg and foot, but also the knee, hips and lower back. Pain often begins in the arch of the foot or the ankle. Blisters may develop on the instep, or on the inside edge of the heels. As overpronation continues and problems develop, pain will be felt elsewhere, depending on the injury.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
Side Step with Opposite Reach. This exercise is designed to load the "bungee cord system" of the gluteal muscle and its opposite, latissimus dorsi muscle to keep the foot from overpronating. Because the opposite arm swings across the front leg when walking, this exercise creates tension in the muscles all the way from the front foot, across the back of the hips and back, to the fingers of the opposite hand. Movement Directions. Stand with left foot on top of the dome of the BT. (Note: For added balance, the right foot can tap on the ground, if needed). Reach right leg out to the side of the BT, and tap the ground while squatting down on the left side and reaching right arm across the left knee. Push down with left big toe while squatting. This activates the arch of the left foot and strengthens all the stabilizing muscles on the left side of the lower body. Return to starting position. Perform 8 to 10 repetitions on each leg.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
The problem with pronation is when it is excessive, here the term overpronation (or hyper-pronation) is used. This is quite a common problem and can lead to a number of injuries, especially in runners, including shin splints, anterior compartment syndrome, patello-femoral pain syndrome, plantar fasciitis, tarsal tunnel syndrome, bunions (Hallux valgus) and achilles tendonitis.
Causes
A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development.
Symptoms
Because overpronation affects the entire lower leg, many injuries and conditions may develop and eventually cause problems not only in the leg and foot, but also the knee, hips and lower back. Pain often begins in the arch of the foot or the ankle. Blisters may develop on the instep, or on the inside edge of the heels. As overpronation continues and problems develop, pain will be felt elsewhere, depending on the injury.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
Side Step with Opposite Reach. This exercise is designed to load the "bungee cord system" of the gluteal muscle and its opposite, latissimus dorsi muscle to keep the foot from overpronating. Because the opposite arm swings across the front leg when walking, this exercise creates tension in the muscles all the way from the front foot, across the back of the hips and back, to the fingers of the opposite hand. Movement Directions. Stand with left foot on top of the dome of the BT. (Note: For added balance, the right foot can tap on the ground, if needed). Reach right leg out to the side of the BT, and tap the ground while squatting down on the left side and reaching right arm across the left knee. Push down with left big toe while squatting. This activates the arch of the left foot and strengthens all the stabilizing muscles on the left side of the lower body. Return to starting position. Perform 8 to 10 repetitions on each leg.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
What Is Severs Disease?
Overview
One of the most common complaints of youth athletes is heel pain. This generally occurs during the early portion of the growth phase around 8-10 years old, and can recur towards the end of growth, (14-16 years old). Symptoms are typically in the back portion of the heel, can occur unilaterally or bilaterally, usually having a gradual onset. The heel bone?s growth plate is in this area, which is immature soft bone and cartilage. A ?tug of war? occurs in this region from the foot growing longer and the leg bones getting taller, which puts tension on this heel bone area known as the calcaneal apophysis. The inflammation is called calcaneal apophysitis or ?Sever?s disease?.
Causes
Sever?s disease is most likely to occur during the growth spurt that occurs in adolescence. For girls, growth spurts usually occurs between 8 and 13 years of age. For boys, it?s typically between 10 and 15 years of age. The back of the heel hardens and becomes stronger when it finishes growing, which is why Sever?s rarely occurs in older adolescents and teenagers.
Symptoms
The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches). During the acute phase of Sever's disease a small heel rise or shock-absorbing heel cup placed under the heel pad of your child's foot may help to ease the symptoms. Your podiatrist or physiotherapist can assess your child's arch and guide you in the best management of your child's condition. We recommend that your child should never go barefooted during the painful stages of Sever's disease.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
One of the most common complaints of youth athletes is heel pain. This generally occurs during the early portion of the growth phase around 8-10 years old, and can recur towards the end of growth, (14-16 years old). Symptoms are typically in the back portion of the heel, can occur unilaterally or bilaterally, usually having a gradual onset. The heel bone?s growth plate is in this area, which is immature soft bone and cartilage. A ?tug of war? occurs in this region from the foot growing longer and the leg bones getting taller, which puts tension on this heel bone area known as the calcaneal apophysis. The inflammation is called calcaneal apophysitis or ?Sever?s disease?.
Causes
Sever?s disease is most likely to occur during the growth spurt that occurs in adolescence. For girls, growth spurts usually occurs between 8 and 13 years of age. For boys, it?s typically between 10 and 15 years of age. The back of the heel hardens and becomes stronger when it finishes growing, which is why Sever?s rarely occurs in older adolescents and teenagers.
Symptoms
The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches). During the acute phase of Sever's disease a small heel rise or shock-absorbing heel cup placed under the heel pad of your child's foot may help to ease the symptoms. Your podiatrist or physiotherapist can assess your child's arch and guide you in the best management of your child's condition. We recommend that your child should never go barefooted during the painful stages of Sever's disease.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
What Will Be The Causes And Signs Or Symptoms Of Achilles Tendon Rupture
Overview
 The Achilles tendon is the largest and strongest tendon in the body. It functions to help control the foot when walking and running. Ruptures of the Achilles tendon commonly occur in individuals in their 30s and 40s. This age group is affected because these patients are still quite active, but over time their tendons tend to become stiffer and gradually weaken. These ruptures usually occur when an athlete loads the Achilles in preparation to pushing off. This can occur when suddenly changing directions, starting to run, or preparing to jump. These ruptures occur because the calf muscle generates tremendous force through the Achilles tendon in the process of propelling the body. Patients will feel a sharp intense pain in the back of their heel. Patients often initially think that they were ?struck in the back of the heel? and then realize that there was no one around them. After the injury, patients will have some swelling. If they can walk at all, it will be with a marked limp. It is very rare that a rupture of the Achilles is partial. However, a painful Achilles tendonitis or a partial rupture of the calf muscle (gastrocnemius) as it inserts into the Achilles can also cause pain in this area. The pain of an Achilles rupture can subside quickly and this injury may be misdiagnosed in the Emergency Department as a sprain. Important clues to the diagnosis are an inability to push off with the foot and a visible or palpable defect just above the heel bone in the back of the leg.
The Achilles tendon is the largest and strongest tendon in the body. It functions to help control the foot when walking and running. Ruptures of the Achilles tendon commonly occur in individuals in their 30s and 40s. This age group is affected because these patients are still quite active, but over time their tendons tend to become stiffer and gradually weaken. These ruptures usually occur when an athlete loads the Achilles in preparation to pushing off. This can occur when suddenly changing directions, starting to run, or preparing to jump. These ruptures occur because the calf muscle generates tremendous force through the Achilles tendon in the process of propelling the body. Patients will feel a sharp intense pain in the back of their heel. Patients often initially think that they were ?struck in the back of the heel? and then realize that there was no one around them. After the injury, patients will have some swelling. If they can walk at all, it will be with a marked limp. It is very rare that a rupture of the Achilles is partial. However, a painful Achilles tendonitis or a partial rupture of the calf muscle (gastrocnemius) as it inserts into the Achilles can also cause pain in this area. The pain of an Achilles rupture can subside quickly and this injury may be misdiagnosed in the Emergency Department as a sprain. Important clues to the diagnosis are an inability to push off with the foot and a visible or palpable defect just above the heel bone in the back of the leg.
Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are corticosteroid medication (such as prednisolone), mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing?s syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture, for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE) - lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel, an inability to bend your foot downward or "push off" the injured leg when you walk, an inability to stand on your toes on the injured leg, a popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward.
Diagnosis
Your caregiver will ask what you were doing at the time of your injury. You may need any of the following. A calf-squeeze test is used to check for movement. You will lie on your stomach on a table or bed with your feet hanging over the edge. Your caregiver will squeeze the lower part of each calf. If your foot or ankle do not move, the tendon is torn. An x-ray will show swelling or any broken bones. An ultrasound uses sound waves to show pictures of your tendon on a monitor. An ultrasound may show a tear in the tendon. An MRI takes pictures of your tendon to show damage. You may be given dye to help the tendon show up better. Tell the caregiver if you have ever had an allergic reaction to contrast dye. Do not enter the MRI room with anything metal. Metal can cause serious injury. Tell the caregiver if you have any metal in or on your body.
Non Surgical Treatment
Once a diagnosis of Achilles tendon rupture has been confirmed, a referral to an orthopaedic specialist for treatment will be recommended. Treatment for an Achilles tendon rupture aims to facilitate the torn ends of the tendon healing back together again. Treatment may be non-surgical (conservative) or surgical. Factors such as the site and extent of the rupture, the time since the rupture occurred and the preferences of the specialist and patient will be considered when deciding which treatment will be undertaken. Some cases of rupture that have not responded well to non-surgical treatment may require surgery at a later stage. The doctor will immobilise the ankle in a cast or a special hinged splint (known as a ?moon boot?) with the foot in a toes-pointed position. The cast or splint will stay in place for 6 - 8 weeks. The cast will be checked and may be changed during this time. 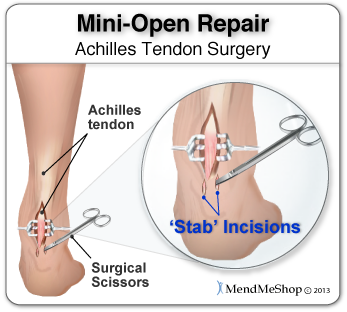
Surgical Treatment
Operative treatment involves a 6cm incision along the inner side of the tendon. The torn ends are then strongly stitched together with the correct tension. After the operation a below knee half cast is applied for 2 weeks. At 2 weeks a brace will be applied that will allow you to move the foot and fully weight-bear for a further 6 weeks. After this you will need physiotherapy. Surgery carries the general risks of any operation but the risk of re-rupture is greatly reduced to 2%. The best form of treatment is controversial with good results being obtained by both methods but surgery is generally recommended for patients under 60 years of age who are fit and active with an intra-substance tear.